
Muscular system of preschool children. Muscular system of a child. Volume of active and passive movements
Children's muscular systems are very different from adults. But for comparison, you need to know anatomy, physiology and biochemistry, but this is not so important in comparison to what you need to know about the characteristics of the child’s muscular system.
In a child, muscle development occurs unevenly. First, the large muscles of the shoulders and forearms develop, then the muscles of the hands. For this reason, children under 6 years old have a hard time doing fine finger work. At the age of 6-7 years, it is much easier for a child to engage in writing, drawing, weaving, modeling, etc. At 8-9 years old, children begin to strengthen ligaments and increase muscle mass, and by the end of puberty, the foundation of muscle status is laid. After the age of 15, small muscles begin to develop intensively again, which help to perfect small movements - coordination and accuracy.
Motor skills in children develop spasmodically, and not evenly. For example, at the age of 10-12 years, coordination of movements is quite good, but prolonged muscle tension, as well as prolonged physical work, do not have high productivity. Also, during puberty, the harmony of movements is disrupted, which is due to the intensive growth of muscle mass and a lag in the function of their regulation.
One of the main conditions for the proper development of a child is a well-formed and functioning support and motor system. By the time of birth, the structural differentiation of the skeletal system is not complete. A peculiarity of bone tissue in children is that the epiphyses of the tubular bones, bones of the hand and foot consist of cartilaginous tissue.
The first ossification nuclei in cartilaginous tissue are formed at the 7-8th week of intrauterine development of the embryo. After the birth of a child, the bone skeleton increases, and at the same time the structure of the bone tissue is rebuilt. In the fetus and newborn it has a fibrous structure; by the age of 3-4 years the bone structure becomes lamellar.
The bone tissue of children contains more water and organic substances and less mineral substances. These features distinguish the bones of a child from the bones of an adult; in a child they are more pliable and elastic under pressure and bending. They have less fragility. Due to the thicker periosteum, fractures in children are often subperiosteal.
Their bone growth occurs due to a good blood supply. After the appearance of ossification points, bone elongation occurs due to the growth cartilaginous tissue, which is located between the ossified epiphysis and metaphysis. The growth of bones in thickness occurs due to the periosteum, while on the side of the bone marrow space there is an increase in the size of the bone in diameter.
Features of the skullin children
The skull of a newborn has a more developed brain part compared to the facial part and consists of paired and unpaired bones, which are separated by sutures. The sutures close by the neonatal period and heal completely by the age of 7 years. Where the bones connect, fontanelles form in certain places:
1) large - between the frontal and parietal bones, size 2.5 x 3 cm;
2) small - between the occipital and parietal bones;
3) lateral - two on each side.
If early closure of the large fontanelle and fusion of the sutures occur, this may indicate microcephaly.
Features of the spinebaby
The spine in newborns has no bends, it is straight, with a slight convexity posteriorly. As motor skills develop, the curves of the spine also develop:
1) cervical lordosis (anterior bending) occurs when the child begins to hold his head up;
2) thoracic kyphosis (posterior bending) occurs when the child sits up on his own;
3) lumbar lordosis appears after 9-12 months, when the child begins to walk.
Thoracic kyphosis is finally formed at 6-7 years, lumbar lordosis - at school age. At the age of 5-6 years, the center of gravity is below the navel, and by the age of 13 years - below the level of the iliac crests.
Features of the child's chest
In the first year of life, a child’s chest has a barrel-shaped shape: wide, the ribs are located horizontally. When the child has learned to walk, the sternum drops somewhat and the ribs acquire an inclined position. The child’s ribs bend easily, the depth of the child’s inhalation depends on the excursion of the diaphragm.
Features of a child's tubular bones
In a child, the tubular bones consist of certain parts. The diaphysis and epiphysis are connected to each other by a layer of metaphyseal cartilage. In these places there is a rich blood supply and slow blood flow, which ensures the formation of tubular bones.
Features of the child's pelvic bones
The pelvic bones in children of the first year of life look like a funnel. The female and male pelvic bones develop during puberty.
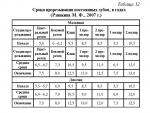
Teeth. First, the child’s milk teeth erupt (see Tables 11, 12).
The level of biological maturity is assessed based on the timing of the eruption of permanent teeth. The number of permanent teeth that have appeared is calculated in total on the upper and lower jaws.

A smaller number of teeth indicates a slower rate of development of permanent teeth.
The formation of the bite also occurs in a certain sequence.
The bite of baby teeth is formed by 2.5 years. It is characterized by: small spaces between the teeth, absence of tooth wear, the distal surfaces of the upper and lower incisors are located in the same frontal plane, the upper incisors slightly cover the lower ones.
At the age of 3.5-6 years, interdental gaps appear, the teeth are worn out, the lower and upper teeth do not match. A straight bite appears. The primary dentition is important for the development of speech and the ability to chew food.
After permanent teeth begin to erupt, a mixed bite appears when the first permanent teeth begin to appear and baby teeth begin to fall out.
At the age of 5, the first permanent teeth appear; at the age of 11, the second molars erupt. Third molars appear between 17 and 20 years of age.
There is a formula for teething:
where n is the child’s age.
The examination of the skeletal system is carried out by examination, which is carried out from top to bottom. In this case, attention is paid to the shape and symmetry, the participation of the chest in the act of breathing, and the presence of skeletal deformation. The child's posture is assessed when he is standing. In case of poor posture, there is a lateral curvature of the spine - scoliosis.
When examining the upper and lower extremities, their length and the presence of deformities are determined.
The examination of the skeletal system is carried out in a certain sequence: from the front, from the side, from the back, and gait disturbance is also determined.
Based on the results of the inspection, a test card is drawn up.

Based on the testing results, the following conclusions are drawn:
1) without deviations, when all points have a negative result;
2) minor deviations with positive answers according to items 3-7;
3) significant deviations with positive answers according to items 1, 2, 8, 9, 10. In these cases, consultation with an orthopedist and a more detailed examination using x-ray analysis are necessary.
Features of the development of the child’s muscular system
In the embryo, muscles begin to develop in the 6th-7th week of pregnancy. Until the age of 5 years, the child’s muscles are not sufficiently developed; the muscle fibers are short, thin, tender and can hardly be felt in the subcutaneous fat layer.
Children's muscles grow during puberty. In the first year of life they make up 20-25% of body weight, by 8 years - 27%, by 15 years - 15-44%. An increase in muscle mass occurs due to a change in the size of each myofibril. An age-appropriate motor regimen plays an important role in muscle development, and at older ages, playing sports.
Training, repetition, and improving quick skills play an important role in the development of children's muscle activity. As the child grows and muscle fiber develops, the intensity of muscle strength increases. Indicators of muscle strength determined using dynamometry. The greatest increase in muscle strength occurs at the age of 17-18 years.
Different muscles develop unevenly. In the first years of life, large muscles of the shoulders and forearms are formed. Up to 5-6 years, motor skills develop; after 6-7 years, the ability to write, sculpt, and draw develops. From 8-9 years of age, the volume of the muscles of the arms, legs, neck, and shoulder girdle increases. During puberty, there is an increase in the volume of the muscles of the arms, back, and legs. At 10-12 years of age, coordination of movements improves.
During puberty, due to an increase in muscle mass, angularity, awkwardness, and abruptness of movements appear. Physical exercises during this period should be of a strictly defined volume.
In the absence of motor load on the muscles (hypokinesia), a delay in muscle development occurs, and obesity, vegetative-vascular dystonia, and impaired bone growth may develop.
For various sports, there is an acceptable age for participating in competitions at a children's sports school.
At 7-8 years old, sports, rhythmic gymnastics, mountain skiing, and figure skating are allowed.
From the age of 9, trampoline classes, biathlon, Nordic combined, ski jumping, and chess are allowed.
At the age of 10, you are allowed to start playing volleyball, basketball, wrestling, rowing, handball, fencing, football, and hockey.
At the age of 12 - boxing, cycling.
At the age of 13 - weightlifting.
At the age of 14 - skeet shooting.
Study of the child's muscular system
The muscular system is examined visually and instrumentally.
The degree and uniformity of development of muscle groups, their tone, strength, and motor activity are assessed visually and palpably.
Muscle strength in young children is determined by attempting to take away a toy. In older children, manual dynamometry is performed.
During an instrumental examination of the muscular system, mechanical and electrical excitability is measured using electromyographs and chronaximometers.
The muscular system is organically connected with the skeletal system, since they jointly provide human movement.
The muscular system in children is poorly developed. The weight of muscles in relation to the weight of the whole body in children is less than in adults, as can be seen from the following data:
- in a newborn - 23.3%;
- for a child 8 years old - 27.2%;
- for a 15-year-old teenager - 32.6%;
- for young men 17-18 years old - 44.2%.
Children's muscles differ in their structure, composition and functions from the muscles of an adult. The muscles in children are paler and more tender in appearance, richer in water, but poorer in protein and fat, as well as extractive and inorganic substances. Only by the age of 15-18 does the amount of water in the muscles decrease, they become denser, and the content of protein, fat and inorganic substances in them increases. At this age, the mass of tendons also increases compared to muscles, and therefore their elasticity and elasticity increase.
Children's muscle development is uneven. They develop larger muscles, such as those in the shoulder and forearm, first, with smaller muscles developing later. Thus, a 4-5 year old child has relatively developed muscles of the shoulder and forearm, but the muscles of the hand are still far from developed, and therefore fine finger work at this age is not yet available to children. The qualitative function of the muscles of the hand develops sufficiently in a child at the age of 6-7 years, when children can already engage in work such as weaving, modeling and other exercises with low-resistance material. The development of the muscles of the hand at this age makes it possible to gradually teach the child to write. But writing exercises at this age should be short-term, so as not to tire the still far from strong muscles of the hand.
An increase in the rate of development of all muscles and an increase in muscle strength in children is observed after 8-9 years, when ligaments are also strengthened and a significant increase in muscle volume is noted. In subsequent years, muscle strength increases steadily. Muscle strength increases especially rapidly in adolescents at the end of puberty. During these same years, an intensive increase in muscle mass occurs.
At the end of puberty, not only does the strength of the arm muscles increase, but the muscles of the back, shoulder girdle and legs also develop powerfully. According to Dementiev's research, the greatest increase in dead strength occurs between the ages of 15 and 18 years. After 15 years, small muscles also develop intensively, due to which the accuracy and coordination of small movements are improved and economy of movements is achieved, which makes it possible to achieve the greatest results with the least expenditure of effort during physical (manual) labor. At the same time, movement technique is also improved.
In children and adolescents, fatigue of working muscles occurs more quickly than in adults. But at the same time, muscle fatigue in children goes away faster, since this is favored by faster metabolism and a more abundant supply of oxygen to them, which restores the excitability of the tired muscle and increases its temporarily weakened elasticity. All this suggests that when organizing and conducting physical exercises, sports activities and physical labor for children and adolescents, it is necessary not to overly burden their muscles, dose the load and conduct these activities at a slow pace with appropriate pauses for rest.
The development of motor skills in children and adolescents does not occur evenly, but spasmodically. By the age of 6-7, the child already has fluent control of his muscles, but precise movements are still difficult for him and are accompanied by great effort. When a child is forced to make precise movements, he quickly gets tired. Imperfect movements in children at this age depend on the insufficient development of coordination mechanisms in the central nervous system.
Coordination of movements, expressed in their accuracy and dexterity, becomes more perfect in children aged 8-12 years. At the same time, children’s mobility increases and their movements become more varied. However, children of primary and partly middle school age are still not capable of long-term productive physical work and prolonged muscle tension. This circumstance must be taken into account when organizing physical education classes and work activities for children.
By the age of 10-13, the child already has some harmony of movements. But during puberty, this harmony is disrupted, since at this time the teenager’s motor apparatus is rebuilt. In this regard, primitive mechanisms (movements) are released from regulation by the higher parts of the central nervous system. Outwardly, in adolescents this manifests itself in an abundance of movements, awkwardness, some angularity, lack of coordination and impaired inhibition. By the end of puberty, these deficiencies in the adolescent’s motor skills are leveled out, and the development of the motor system is basically completed.
The above-mentioned features of the development of muscles and motor skills of children and adolescents put forward a number of hygienic requirements aimed, on the one hand, at protecting their muscular system, and on the other, at its development and strengthening. Considering the relatively rapid fatigue of muscles in children and adolescents and their lack of training, it is necessary to avoid prolonged and especially excessive physical stress, keeping in mind the possible dire consequences that can lead to crippling of a growing organism and a delay in its development. This applies not only to children of preschool and primary school age, but also to adolescents studying in high school and vocational schools.
To ensure normal muscle development in children and adolescents, moderate physical exercise is necessary, be it sports, agricultural or other physical labor. When working, muscles receive a more abundant flow of blood containing nutrients and oxygen. The blood that flows into a muscle when it works nourishes not only it, but also the bones to which it is attached, as well as ligaments. Muscle work also has a positive effect on the formation of red blood cells in the bone marrow, thereby improving the composition of the blood. Muscular work has a beneficial effect on the entire body, in particular on organs such as the heart and lungs, and activates metabolic processes.
The activity of muscles is organically connected with the work of the brain and nerves, which mutually influence each other. As noted above, muscle exercise promotes the development of the cerebral cortex. The education of mental qualities, such as perception, memory, will, is associated with rational physical education. The work of the brain is more productive when its nutrition with blood delivered to it is enhanced. Thus, moderate physical exercise activates mental activity. However, with excessive muscle contractions, fatigue occurs not only in the muscles, but also in the nervous system.
Excessive muscle tension, especially when it occurs for a long time, has a harmful effect on the functioning of the entire body and can lead to serious diseases of the heart, lungs and other organs. With such excessive prolonged muscle tension, the heart works much more intensely, the heart muscle gets tired, as a result of which its contractions become slower. With prolonged tension in the muscles of the hands when playing the piano, sewing and writing, a disease known as writer's cramp sometimes occurs, which is expressed by severe pain in the muscles of the hand and the inability to continue working. All this must be kept in mind when conducting educational work with children and adolescents.
However, not only excessive prolonged muscle tension has an adverse effect on the body, but also insufficient work of individual muscle groups. The consequence of this is disorders in individual parts of the body, affecting the entire body. Thus, with a prolonged stationary sitting position without breaks for active rest in the form of movements of the whole body, the blood circulation of the abdominal organs (stomach, intestines and liver) is disrupted, which can result in constipation. Therefore, it is so important during sedentary work to arrange breaks for rest, which should be accompanied by free movements of all the muscles of the body as much as possible. Such rest after prolonged stationary sedentary work will be much more effective if it is carried out in the fresh air.
The most important thing in the hygiene of the muscular system of children and adolescents is its exercise, training, which gradually involves individual muscle groups (in their mutual connection) in movements and thereby ensures the development of muscles and improves motor skills. Learning new movements, for example, during the initial training in writing, gymnastics, playing musical instruments, and certain types of physical labor, requires children not only to spend significant amounts of muscle, but also to experience considerable neuropsychic stress, which entails physical and mental fatigue. Systematic, gradually increasing, but at the same time strictly dosed training of individual muscle movements in the process of learning the above activities makes these movements familiar, easy and enjoyable. If these activities are not excessive in time and load, then they usually do not cause fatigue in a trained child and teenager. In connection with the above, the enormous hygienic and pedagogical importance of training the muscular system becomes obvious.
From a hygienic point of view, it is extremely important to ensure the comprehensive development of the muscles of children and adolescents and to avoid unilateral stress on one or another muscle group. With a unilateral load on any one muscle group, its excessive development occurs due to some underdevelopment of the remaining muscle groups, and this circumstance negatively affects the activity of the entire organism. Only comprehensive muscle exercise ensures the normal physical development of the growing organism as a whole and contributes to the improvement of the morphological and functional properties of individual organs and systems.
At primary school age, the main type of physical exercise is outdoor games. At this age, some strength exercises are already available, but only those that do not require strong tension. Gymnastic exercises at primary school age become more important compared to preschool age, but they are not yet the main type of physical education for children in this period. Only in middle and high school age do gymnastics and sports become the main types of physical education among adolescents, since at this age the muscular system has developed sufficiently for this kind of exercise.
When addressing issues of physical education among children and adolescents, it is not enough to take into account only the characteristics of the skeletal and muscular systems. In this regard, the characteristics of the cardiovascular system of children and adolescents are of great importance. Only taking into account all factors of the development of the body can ensure the correct organization of educational work among children and adolescents and the implementation of activities among them in the field of individual hygiene.
The first 7 years of a child’s life are characterized by intensive development of all organs and systems. A child is born with certain inherited biological properties, including typological features of the basic nervous processes (strength, balance and mobility). But these features are only the basis for further physical and mental development, and the determining factor from the first months of life is the child’s environment and upbringing. Therefore, it is very important to create such conditions and organize education in such a way that a cheerful, positive emotional state of the child and full physical and mental development are ensured.
The muscular system of a young child is not yet sufficiently developed compared to an adult, and muscle mass makes up about 25% of his body weight, while in an adult it is on average 40-43%.
As the child develops movements, the mass and contractility of muscle tissue increase. The increase in muscle strength is largely determined by gradually increasing physical activity during physical exercise.
In children of primary preschool age, the extensor muscles are not sufficiently developed and are quite weak, so the child often takes incorrect postures - a lowered head, cramped shoulders, a stooped back, a sunken chest. By the age of 5, muscle mass increases significantly, especially the muscles of the lower extremities, and the strength and performance of muscles increases. Indicators of muscle strength reflect both the characteristics of age-related development and the influence of physical education. The strength of the hand muscles increases from 3.5-4.0 kg at the age of 3-4 years to 13-15 kg by the age of 7 years. Already from the age of 4, differences in the performance of boys and girls are noted. The strength of the trunk muscles (dead strength) by the age of 7 almost doubles from 15-17 kg at 3-4 years to 32-34 kg.
The static state of muscles is usually called muscle tone. Muscle tone is maintained by impulses coming from the central nervous system. In the first months of life in children, the tone of the flexor muscles of the limbs prevails over the tone of the extensors, which determines the characteristic posture of an infant. The muscle tone of the upper extremities usually levels out by 2.5-3 months, and the muscle tone of the lower extremities by 3-4 months. In case of illness (rickets, hypotrophy), these periods may change. In young children, muscle tone at rest decreases under the influence of massage and gymnastics.
The state of muscle tone in preschool age is of great importance for the formation of correct posture. Of particular importance is the tone of the trunk muscles, which create a natural “muscle corset”.
With age, there is an increase in the tension tone of the muscles of the back and abdomen, which is the result of not only an improvement in the regulatory function of the central nervous system, but also the positive effect of physical exercise training.
Jumping plays a special role in the development of strength, so it is necessary to form the basics of technique when performing a jump, since technique helps to correctly distribute the strength of the leg muscles when pushing off, and the strength of the arm and back muscles.
So, the muscular system of a young child is not yet sufficiently developed, therefore, as the child’s movements develop, the mass and contractility of muscle tissue increases. The increase in muscle strength is largely determined by gradually increasing physical activity.
Propaedeutics of childhood diseases: lecture notes by O. V. Osipov
2. Anatomical and physiological features of the muscular system in children
Muscle mass in relation to body weight in children is significantly less than in adults. The distribution of muscle tissue in a newborn differs from children of other age groups and adults. Its bulk falls on the muscles of the trunk, while in other periods it falls on the muscles of the limbs.
A feature of newborns is a significant predominance of flexor muscle tone. Due to the increase in flexor tone in the prenatal period, a specific fetal position occurs.
In parallel with the development of muscle fibers, the formation of a connective tissue framework of muscles (endomysium and perimysium) occurs, which reaches the final degree of differentiation by 8-10 years.
In newborns (unlike adults), even during sleep, the muscles do not relax. The constant activity of skeletal muscles is determined, on the one hand, by their participation in the reactions of contractile thermogenesis (heat production), and on the other, by the participation of this activity and muscle tone in the anabolic processes of the growing organism (primarily in stimulating the development of muscle tissue itself).
Muscle development in children is uneven. First of all, the large muscles of the shoulder and forearm develop, and later the muscles of the hand. Children under 6 years old cannot do fine work with their fingers. At the age of 6–7 years, a child can already successfully engage in such work as weaving, modeling, etc. At this age, children can gradually learn to write. However, writing exercises should be short-term, so as not to tire the still weak muscles of the hands.
From the age of 8–9 years, children already have stronger ligaments, increased muscle development, and a significant increase in muscle volume. At the end of puberty, muscle growth occurs not only in the arms, but also in the muscles of the back, shoulder girdle and legs.
After 15 years, small muscles also develop intensively, and the accuracy and coordination of small movements improves.
Moderate physical exercise is necessary for normal muscle development in children and adolescents.
From the book Children's Diseases. Complete guide author author unknownPART I ANATOMICAL AND PHYSIOLOGICAL FEATURES OF CHILDREN
From the book Propaedeutics of Childhood Illnesses by O. V. OsipovaCHAPTER 2. ANATOMICAL AND PHYSIOLOGICAL FEATURES OF THE MUSCULOSCULAR SYSTEM One of the main conditions for the proper development of a child is a well-formed and functioning musculoskeletal system. By the time of birth, structural differentiation of the skeletal system
From the book Propaedeutics of Childhood Illnesses: Lecture Notes by O. V. OsipovaCHAPTER 4. ANATOMICAL AND PHYSIOLOGICAL FEATURES OF THE RESPIRATORY SYSTEM The formation of the tracheopulmonary system begins at the 3-4th week of embryonic development. Already by the 5-6th week of embryo development, second-order branches appear and it is predetermined
From the author's bookANATOMICAL AND PHYSIOLOGICAL FEATURES OF THE HEART AND VESSELS IN CHILDREN Children experience continuous growth and functional improvement of the cardiovascular system. The heart grows and improves especially vigorously in children from 2 to 6 years of age, as well as during puberty.
From the author's bookCHAPTER 6. ANATOMIC AND PHYSIOLOGICAL FEATURES OF THE DIGESTIVE SYSTEM IN CHILDREN The digestive organs include the oral cavity, esophagus, stomach and intestines. The pancreas and liver take part in digestion. The digestive organs are formed in the first 4 weeks
From the author's book15. Anatomical and physiological features of the musculoskeletal system The formation and formation of bone tissue occurs in the 5th week of intrauterine development. By the time the child is born, the skull is represented by a large number of bones. The sagittal, coronal and occipital sutures are open and
From the author's book17. Anatomical and physiological features of the respiratory system The right lung consists of three lobes: upper, middle and lower, and the left lung consists of two: upper and lower. The middle lobe of the right lung corresponds to the lingular lobe in the left lung. Along with the division of the lungs into lobes, a large
From the author's book27. Anatomical and physiological features of the digestive system Research methods The digestive organs include the oral cavity, esophagus, stomach, duodenum, small intestine, large intestine (cecum, transverse colon, sigmoid, rectum),
From the author's book30. Anatomical and physiological features of the excretory system The kidneys perform two main functions: 1) regulate the composition of extracellular fluid and the acid-base state of the body; 2) ensure the removal of toxic substances or products from the body
From the author's book1. Anatomical and physiological features of the nervous system in children The formation of the nervous system occurs in the 1st week of intrauterine development. The greatest intensity of division of nerve cells in the brain occurs in the period from 10 to 18 weeks of intrauterine development,
From the author's bookLECTURE No. 7. Anatomical and physiological features of the musculoskeletal system and semiotics of lesions 1. Anatomical and physiological features of the skeletal system The laying and formation of bone tissue occurs in the 5th week of intrauterine development. Bone tissue is very
From the author's book1. Anatomical and physiological features of the skeletal system The formation and formation of bone tissue occurs in the 5th week of intrauterine development. Bone tissue is very sensitive to adverse environmental influences, especially to nutritional disorders,
From the author's bookLECTURE No. 8. Anatomical and physiological features of the respiratory system in children. Lesion syndromes and research methods 1. Anatomical and physiological features of the respiratory system in children. Research technique The right lung consists of three lobes: upper, middle and lower, and
From the author's book1. Anatomical and physiological features of the respiratory system in children. Research technique The right lung consists of three lobes: upper, middle and lower, and the left lung consists of two: upper and lower. The middle lobe of the right lung corresponds to the lingular lobe in the left lung. Along with
From the author's bookLECTURE No. 12. Anatomical and physiological features of the endocrine system in children. Sexual development. Semiotics of lesions 1. Anatomical and physiological features of the endocrine system in children. Sexual development The pituitary gland is the most important endocrine gland that produces
From the author's book1. Anatomical and physiological features of the endocrine system in children. Sexual development The pituitary gland is the most important endocrine gland, producing a number of tropic protein hormones. Connected with the hypothalamic region of the central nervous system. Exerts a regulatory effect





 Ustyugov refused the Tour de Ski
Ustyugov refused the Tour de Ski Why remove gills from fish for soup?
Why remove gills from fish for soup? Horse and Dragon: compatibility in friendship, love and business
Horse and Dragon: compatibility in friendship, love and business What documents are needed to obtain a fan ID?
What documents are needed to obtain a fan ID?